CAN ATHLETES FAVORABLY ALTER BODY COMPOSITION WITH EPHEDRINE, CAFFEINE AND ASPIRIN?
Michael C. Prevost
Aerospace Physiologist - Marine Aircraft Group 39, Camp Pendleton, CA.
Key Words: ephedrine, caffeine, aspirin, beta agonist, sympathetic nervous system, stimulants
Abstract
Can athletes favorably alter body composition with ephedrine, caffeine and aspirin? J. Perf. Enhan. 1999 1(1):31-43. The sympathetic nervous system plays a direct role in the control of thermogenesis and the control of energy balance in the body. Evidence indicates that some cases of obesity may be due in part to an inadequate sympathetic tone. The sympathetic agonists ephedrine, caffeine and aspirin have been studied extensively to determine the feasibility of using these agents to correct for an inadequate sympathetic tone in obese individuals. Ephedrine alone is fairly ineffective as an anorectic and thermogenic agent. However, the addition of caffeine or caffeine and aspirin greatly enhances both the anorectic and thermogenic properties of ephedrine. The combination has been shown to be effective at producing weight loss and preserving muscle mass in animals and in obese adults on low calorie diets. Most of the weight loss can be accounted for by anorectic effects but thermogenic effects play a role as well. The combination is well tolerated in controlled research studies. However, the FDA is concerned about the over the counter sale of ephedrine following a large number of reports concerning adverse reactions. Because all of the research has been performed on animals or obese adults it is difficult to say if ephedrine, caffeine and aspirin would be beneficial to athletes trying to alter body composition.
Physiology Lesson
The Sympathetic Nervous System
The sympathetic nervous system discharges under emergency situations or under situations of stress or anxiety. It is the sympathetic nervous system that is responsible for the "fight or flight" response. The "fight or flight" response is a short term response that is designed to help prepare us to deal with emergency situations. According to Ganong (1) some of the results of sympathetic nervous system discharge are:
The sympathetic nervous system consists of a series of nerve pathways that originate in the spinal cord from T1 (first thoracic vertebra) to L3 (third lumbar vertebra). These nerves connect with another large grouping of nerves which eventually connect with various organs such as the heart, lungs, muscles, eyes, kidneys, bladder, and many others. The adrenal medulla is also part of the sympathetic nervous system. The adrenal medulla is a large grouping of sympathetic nervous system nerve cells located just above the kidneys that secrete epinephrine (adrenaline) when stimulated. The majority of the nerves in the sympathetic nervous system secrete norepinephrine (noradrenaline). Both norepinephrine and epinephrine have similar effects on the body as listed above.
Epinephrine and norepinephrine affect body tissues by binding to receptors on the outside surfaces of body cells. These receptors can be grouped into two types, Alpha (a ) and Beta (b ). There are at least two subtypes of Alpha receptors (a 1 and 2) and at least 3 subtypes of Beta receptors (b 1,2 and 3). Not all of the cells of the body have receptors for epinephrine and norepinephrine but many do including:
Eyes
Heart
Arterioles
Systemic Veins
Lungs
Stomach
Intestine
Gallbladder
Urinary bladder
Ureter
Uterus
Male sex organs
Spleen
Adrenal medulla
Liver
When one of the sympathetic nervous system hormones (norepinephrine or epinephrine) binds to a b receptor it results in the production of a substance called cyclic AMP inside of the cell. Cyclic AMP is called a "second messenger" because it is produced in response to the "first messenger," norepinephrine or epinephrine (also a host of other hormones) and it serves as a modulator to turn processes on and off. Therefore the hormones norepinephrine and epinephrine exert their effects by increasing the intracellular (inside the cell) concentrations of cyclic AMP.
Cyclic AMP modulates a multitude of processes in the body. Of importance to athletes are the effects on energy metabolism and muscle anabolism. The liver, heart, skeletal muscles and fat cells all have b receptors on their surfaces and the stimulation of these b receptors has a dramatic impact on the functioning of these tissues.
The Heart - The binding of epinephrine or norepinephrine or any synthetic drug that would be considered a b -agonist (A b -agonist is a drug that acts like norepinephrine or epinephrine and binds to b receptors.) results in an increase in cyclic AMP inside the cardiac muscle cells. An increase in cyclic AMP increases the inflow of calcium into cardiac muscle cells. Calcium results in an increase in heart rate and an increase in cardiac muscle contraction force. As a result cardiac output increases (Cardiac output is the amount of blood pumped per unit of time.). Cardiac blood flow (blood flow to cardiac muscle) is also increased because of vasodilation of coronary arteries.
Skeletal Muscle - b receptor activation in skeletal muscle activates glycogenolysis (Glycogenolysis is the breakdown of glycogen into simple sugars to serve as a source of energy for muscle contraction.).
Liver - Circulating b -agonist hormones also stimulate glycogenolysis in liver tissue. This results in a release of glucose into the bloodstream to increase blood sugar. Also, gluconeogenesis is activated in the liver. Gluconeogenesis is the process of making glucose (sugar) from proteins and metabolic by products. This "new" glucose is also used to increase blood sugar to serve as a source of energy.
Fat Cells - b receptor stimulation on the surface of a fat cell results in the activation of an enzyme called hormone sensitive lipase. Hormone sensitive lipase is an enzyme that activates lipolysis (fat breakdown) in the fat cell. This results in the release of fat from the fat cell into the bloodstream to be used as a source of fuel. This is the first step in the process of burning fat. Since fat is stored in fat cells and burned primarily by active muscle cells, this first step is important to get the fat from its storage site to the site where it will be burned.
Peripheral Vasculature – Sympathetic stimulation can either dilate (open up) or constrict peripheral vasculature. b receptors have a greater affinity for sympathetic nervous system hormones but a receptors are dominant. Therefore low concentrations of sympathetic nervous system hormones will stimulate primarily b receptors and result in vasodilation, while high concentrations of these hormones stimulate a receptors as well and result in vasoconstriction. As a result, high concentrations of epinephrine can lead to an increase in blood pressure because it increases cardiac output and resistance to blood flow (by stimulating vasoconstriction).
The Role of Caffeine, Ephedrine and Aspirin
Ephedrine is a drug that can be obtained from a variety of plants in the genus Ephedra. It is considered a nutritional supplement by the FDA and is available over the counter. Ephedrine is a central nervous system stimulant. It stimulates the release of norepinephrine from its peripheral storage sites. It also has direct norepinephrine like effects by binding directly to b receptors.
Figure 1. Ephedrine
Caffeine is an inhibitor of an enzyme called phosphodiesterase (PDE). PDE lowers cyclic AMP concentrations inside the cell by catalyzing the degradation of cyclic AMP. PDE returns cyclic AMP concentrations to normal after b receptor stimulation. If PDE is inhibited by caffeine cyclic AMP concentrations rise. Caffeine may also enhance norepinephrine release from peripheral storage sites.
Caffeine can be found in chocolates, sodas, coffee, tea, guarana, mate and in many over the counter medications such as No Doze and Excedrin. Caffeine has widespread effects in the body including stimulating the respiratory system, central nervous systems, cardiac muscle, and increasing alertness and urine production.
Figure 2 Caffeine
Aspirin inhibits adenosine receptors. The binding of adenosine to its receptor turns off norepinephrine release. As a result consumption of aspirin can result in a greater release of norepinephrine.
Aspirin is the substance in Willow Bark, salicin, which is the pharmacological ancestor of a family of drugs called salicylates. Aspirin is the best known salicylate and the world’s most used drug.
Figure 3 Aspirin
As you can see each of these substances works at a different step in the pathway but all result in an increase in the intracellular concentration of cyclic AMP. Recall that the sympathetic nervous system hormones exert their effects through b receptors by increasing the intracellular concentrations of cyclic AMP. Since each substance works at a different point in the signaling cascade the results are additive. In other words they amplify the effects of one another resulting in dramatically increased sympathetic nervous system stimulation.
Figure 4. Role of Ephedrine, Caffeine and Aspirin
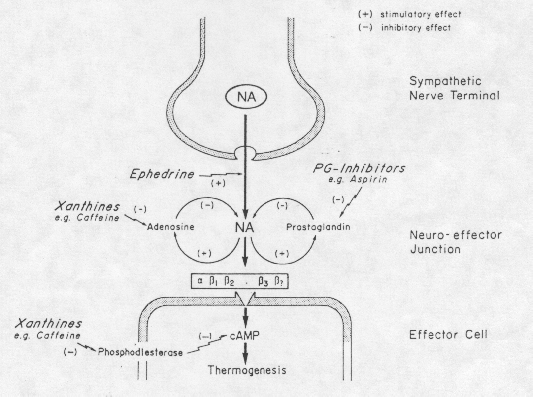
Figure from A. G. Dullo, Int J Obes Relat Metab Disord. 1993 Feb;17 Suppl 1:S35-40.
Review of the Literature
Stimulating the sympathetic nervous system increases whole body caloric expenditure (2). This increased rate of caloric expenditure, if not compensated for by an increase in caloric consumption, should lead to weight loss if caloric expenditure exceeds caloric consumption (if you burn more than you eat). Dulloo and Miller (3) found that administering drugs which both reduce noradrenaline levels and decrease metabolic rate leads to a considerable increase in body fat and propose that this provides considerable support for the concept of an important role of the sympathetic nervous system in the overall control of thermogenesis and in energy balance regulation. Because many obese adults have a reduced capacity for energy expenditure (4) researchers have long sought after a pharmacological treatment approach that increases energy expenditure. Because of their effect on energy expenditure researchers have explored the use of sympathomimetic drugs (drugs that stimulate the sympathetic nervous system like caffeine, aspirin and ephedrine) to enhance weight loss in obese individuals. Of particular interest to researchers were the drugs ephedrine, caffeine and aspirin because their effects are additive, they are cheap and readily available over the counter.
Ephedrine
Although in humans ephedrine administration can stimulate thermogenesis (increased metabolic rate), the administration of ephedrine alone is fairly ineffective at promoting weight loss and has been shown to be as ineffective as a placebo (3). Pasquali et al. (4) showed no significant weight loss over a placebo when subjects were given 150 mg of ephedrine per day for 3 months. Ephedrine alone also fails to increase plasma glycerol and free fatty acid concentrations indicating a negligible effect on lipolysis (5). However, Pasquali et al. (6) found that ephedrine alone (50mg three times daily) did result in lower urinary nitrogen output in obese adults on a very low calorie diet. This is suggestive of a protein sparing effect.
Caffeine
A single oral dose of caffeine (100 mg) has been shown to increase the metabolic rate in humans by 3-4% for over two hours (7). When subjects were given 100 mg doses every 2 hours for a 12 hour period metabolic rate was increased by 8-11%. The researchers calculated that this would result in an increased energy expenditure in lean adults of 150 kcal per day and 79 kcal per day in post obese subjects.
Aspirin
Chronic administration of aspirin alone has no effect on energy expenditure and body composition (8) in experimental animals. However the addition of aspirin to ephedrine results in a doubling of energy expenditure compared to ephedrine alone (8). In one animal study the ephedrine group increased energy expenditure by 9% and reduced body weight and body fat by 18% and 50%, respectively (8). The ephedrine and aspirin group reduced bodyfat by over 75%.
Combinations of Ephedrine, Caffeine and Aspirin
Although ephedrine alone is ineffective at enhancing weight loss, Astrup et al. demonstrated that the addition of caffeine (20mg ephedrine / 200 mg caffeine) resulted in an extra 3.4 kg (7.5 pounds) weight loss compared to controls (3). Using a dose of 20 mg ephedrine and 200 mg caffeine three times daily for 8 weeks, Astrup et al.
(9) demonstrated a loss of 4.5 kg more body fat and 2.8 kg less fat-free mass in the supplemented group than the placebo group, this suggested that the combination can not only promote fat loss but may also help to preserve fat free mass on a hypocaloric (calorie intake below maintainence levels) diet. In a study at Harvard University researchers investigated the effects of of a mixture of ephedrine (75-150mg), caffeine (150mg) and aspirin (330mg), in divided premeal doses on weight loss in 24 obese adults (10). Over an 8 week period weight loss was 2.2kg (4.8 lbs) for ECA vs. 0.7 kg (1.5 lbs.) for placebo. After 5 months on ephedrine, caffeine and aspirin (ECA), average weight loss in subjects was 5.2 kg (11.5 lbs.) compared to 0.03 kg (.066 lbs.) gained on a placebo. Over this period the researchers reported no significant changes in heart rate, blood pressure, blood glucose, insulin, and cholesterol levels, and no differences in the frequency of side effects between treatment and placebo. In an animal study using obese rats researchers found that the administration of ECA produced a rapid decline in body weight, which reached lean levels within 9-10 weeks. Researchers further found that ECA reduced food intake and minimized the fall in metabolic rate that usually accompanies a reduction in caloric intake.The mechanism of action of the ephedrine, caffeine and aspirin combination is twofold: it stimulates thermogenesis and has anorectic (appetite suppressing) properties. In a review of the pharmacology of thermogenic drugs Astrup et al. (11) calculated that 75% of the weight loss produced by a caffeine/ephedrine combination was due to an anorectic effect and 25% due to a thermogenic effect. Wellman reports that the anorectic effect is due to the stimulation of b receptors in the hypothalamus (12). The hypothalamus is the primary location of the hunger and saiety centers of the brain (1).
The increased thermogenesis in response to ephedrine is due to the stimulation of b 1,2 and 3 receptors (13). Liu et al. (13) showed that 43% of the thermogenic response of ephedrine remained after blocking b 1 and 2 receptors with a blocking agent (nadolol). The researchers proposed that this was due to the stimulation of an atypical receptor, the b 3 receptor. Although the cardiovascular system effects of ECA diminish rapidly, the effects on energy expenditure do not decline with time as often occurs with other drugs (14).
Safety Considerations
Recall, the Harvard University study mentioned earlier (10) found that over a 5 month period there were no significant changes in heart rate, blood pressure, blood glucose, insulin, and cholesterol levels, and no differences in the frequency of side effects between treatment and placebo. In a more recent study Waluga et al. (15) found no significant changes in cardiac functioning at rest when subjects consumed ephedrine (2X 25 mg) and caffeine (2 X 200 mg). They did demonstrate an increased ejection fraction (the % of blood in the left ventricle that is ejected with each heart beat). This is not surprising since b receptor stimulation by norepinephrine or epinephrine leads to this affect as well. In a 50 week study Toubro et al. (16) administered ephedrine and caffeine (20mg/200mg three times daily) for 24 weeks, withdrew the drugs for two weeks, then resumed drug treatment until week 50. They reported that side effects were minor and transient and observed no significant withdrawal symptoms. In an 8 week study Daly et al. (17) found that ECA (150mg/150mg/333mg in divided doses) resulted in no significant changes in heart rate, blood pressure, blood glucose, insulin, and cholesterol levels, and no differences in the frequency of side effects were found.
In 1994 Buemann et al. (18) demonstrated that the combination of ephedrine and caffeine (20mg/200mg three times daily) may have beneficial effects on blood lipids during a low calorie diet. The researchers found that ephedrine and caffeine prevented the decline in HDL cholesterol (the "good" cholesterol) and reduced blood triglycerides when compared to a placebo group.
Some studies have reported significant side effects resulting from supplementing with ECA. Breum et al. (19) reported that 53% of the subjects consuming ephedrine and caffeine (20mg/200mg three times daily) complained of side effects. The most pronounced side effect was agitation. Pasquali et al. (20) found significantly more cardiovascular side effects in a group consuming 150mg of ephedrine daily compared to a 50mg per day group and a placebo group. Also, the FDA has voiced concern over the over the counter sale of ephedrine (21). In an FDA Medical Bulletin reported adverse events such as nervousness, dizziness, tremor, alternations in blood pressure or heart rate, headache, gastrointestinal distress, chest pain, myocardial infarction, hepatitis, stroke, seizures, psychosis, and death. Since 1994 the FDA has received and investigated over 800 adverse events associated with the use of ephedrine (21). It is important to note however that these reports are not from controlled studies and may be the result of drug interactions, hypersensitivity and overdose.
Recommendations and Conclusions
Although ECA increases energy expenditure, reduces appetite and may spare muscle in obese adults on a low calorie diet, there is evidence that lean adults might not respond in the same way to ECA. One study demonstrated that aspirin (300mg) enhanced the thermogenic response of ephedrine (30mg) in obese but not lean women (21). If indeed one of the causes of obesity is a decreased capacity for thermogenesis, agents like ECA that increase thermogenesis might be considered appropriate treatment. In lean adults (specifically lean adults not predisposed to obesity) however, there is presumably no defect in thermogenesis. Therefore drugs that "correct" a decreased capacity for thermogenesis are not appropriate and might not be effective in lean adults. To date, besides the aforementioned study, no study has examined the effectiveness of ECA in lean adults. Therefore it is difficult to speculate on the effectiveness of ECA in altering the body composition of athletes. The safety of the ECA combination remains a question. Although most studies indicate the ECA is well tolerated in healthy adults, the FDA has reported several incidents including seizures, strokes and death. Little is known about the effect of ECA on several medical conditions and whether there are dangerous interactions with other supplements and drugs. Also, the cardiovascular effects of ECA have not been studied under extremely high intensity exertion experienced by competitive athletes during training and competition. Athletes should consider ECA only after a consultation with a physician and proceed with caution. Future studies may answer the questions of safety and efficacy for athletes.
For those athletes that choose to use ECA it is difficult to suggest appropriate dosing strategies. One might speculate that the doses mentioned in this review (20-150mg Ephedrine, 100-200mg Caffeine and 200-330mg Aspirin daily) might be a good place to start. As mentioned earlier, these doses may prove to be ineffective for athletes or unsafe during very demanding, high intensity training and competition settings. The FDA proposed legislation that would require labels to recommend no more than 8mg of ephedrine every 6 hours and no more than 24mg daily (22). The FDA also proposed prohibiting the inclusion of other stimulant ingredients like caffeine with ephedrine.
Developing exclusion criteria for individuals who should not take ECA is also difficult. The FDA reports a large number of adverse events associated with ephedrine use in healthy young adults. Many of these adverse events occurred on the first use or within 2 weeks (23). Also difficult would be developing cessation criteria for those already taking ECA. This is because many potential side effects, like high blood pressure, may not be noticed by the user and other side effects, like myocardial infarction (heart attack) or stroke, may occur suddenly with no warning.
References Cited
1. Ganong, WE Review of Medical Physiology. Appleton & Lange Norwalk, CT San Mateo, CA. 1987.
2. Massoudi M, Evans E, Miller DS, Thermogenic drugs for the treatment of obesity: screening using obese rats and mice. Ann Nutr Metab 1983, 27:26-37.
3. Astrup A, Breum L, Toubro S, Hein P, Quaade F The effect and safety of an ephedrine/caffeine compound compared to ephedrine, caffeine and placebo in obese subjects on an energy restricted diet. A double blind trial. Int J Obes Relat Metab Disord 1992 Apr;16(4):269-77
4. Pasquali R, Baraldi G, Cesari MP, Melchionda N, Zamboni M, Stefanini C, Raitano A A controlled trial using ephedrine in the treatment of obesity.Int J Obes 1985;9(2):93-8
5. Astrup A, Toubro S, Cannon S, Hein P, Madsen J. Thermogenic metabolic and cardiovascular effects of a B-agonist, ephedrine. A double blind placebo-controlled study in humans. Curr Ther Res 1990: 48:1087-1100
6. Pasquali R, Casimirri F, Melchionda N, Grossi G, Bortoluzzi L, Morselli Labate AM, Stefanini C, Raitano A Effects of chronic administration of ephedrine during very-low-calorie diets on energy expenditure, protein metabolism and hormone levels in obese subjects. Clin Sci (Colch) 1992 Jan;82(1):85-92
7. Dulloo AG, Geissler CA, Horton T, Collins A, Miller DS Normal caffeine consumption: influence on thermogenesis and daily energy expenditure in lean and postobese human volunteers. Am J Clin Nutr 1989 Jan;49(1):44-50
8. Dulloo AG, Miller DS Aspirin as a promoter of ephedrine-induced thermogenesis: potential use in the treatment of obesity. Am J Clin Nutr 1987 Mar;45(3):564-9
9. Astrup A, Buemann B, Christensen NJ, Toubro S, Thorbek G, Victor OJ, Quaade F The effect of ephedrine/caffeine mixture on energy expenditure and body composition in obese women. Metabolism 1992 Jul;41(7):686-8
10. Daly PA, Krieger DR, Dulloo AG, Young JB, Landsberg L Ephedrine, caffeine and aspirin: safety and efficacy for treatment of human obesity. Int J Obes Relat Metab Disord 1993 Feb;17 Suppl 1:S73-8
11. Astrup A, Toubro S, Christensen NJ, Quaade F Pharmacology of thermogenic drugs.Am J Clin Nutr 1992 Jan;55(1 Suppl):246S-248S
12. Wellman PJ Overview of adrenergic anorectic agents. Am J Clin Nutr 1992 Jan;55(1 Suppl):193S-198S
13. Liu YL, Toubro S, Astrup A, Stock MJ Contribution of beta 3-adrenoceptor activation to ephedrine-induced thermogenesis in humans. Int J Obes Relat Metab Disord 1995 Sep;19(9):678-85
14. Astrup A, Toubro S Thermogenic, metabolic, and cardiovascular responses to ephedrine and caffeine in man. Int J Obes Relat Metab Disord 1993 Feb;17 Suppl 1:S41-3
15. Waluga M, Janusz M, Karpel E, Hartleb M, Nowak A Cardiovascular effects of ephedrine, caffeine and yohimbine measured by thoracic electrical bioimpedance in obese women. Clin Physiol 1998 Jan;18(1):69-76
16. Toubro S, Astrup AV, Breum L, Quaade F Safety and efficacy of long-term treatment with ephedrine, caffeine and an ephedrine/caffeine mixture. Int J Obes Relat Metab Disord 1993 Feb;17 Suppl 1:S69-72
17. Daly PA, Krieger DR, Dulloo AG, Young JB, Landsberg L Ephedrine, caffeine and aspirin: safety and efficacy for treatment of human obesity. Int J Obes Relat Metab Disord 1993 Feb;17 Suppl 1:S73-S78
18. Buemann B, Marckmann P, Christensen NJ, Astrup A The effect of ephedrine plus caffeine on plasma lipids and lipoproteins during a 4.2 MJ/day diet. Int J Obes Relat Metab Disord 1994 May;18(5):329-332
19. Breum L, Pedersen JK, Ahlstrom F, Frimodt-Moller J Comparison of an ephedrine/caffeine combination and dexfenfluramine in the treatment of obesity. A double-blind multi-centre trial in general practice. Int J Obes Relat Metab Disord 1994 Feb;18(2):99-103
20. Horton TJ, Geissler CA Aspirin potentiates the effect of ephedrine on the thermogenic response to a meal in obese but not lean women. Int J Obes 1991 May;15(5):359-366
21. U. S. Food and Drug Administration, Adverse Events with Ephedra and Other Botanical Dietary Supplements FDA Medical Bulletin September 1994, From the World Wide Web at:
http://vm.cfsan.fda.gov/~dms/ds-ephe2.html22. HHS News, US Department of Health and Human Services, June 2, 1997, From the World Wide Web at: http://vm.cfsan.fda.gov/~lrd/hhsephed.html.
23. Federal Register: June 4, 1997 (Volume 62, Number 107), From the World Wide Web at: http://vm.cfsan.fda.gov/~lrd/fr97064a.html.
Glossary of Terms:
anorectic – a substance that reduces the appetite
thermogenesis – the generation of heat
agonist – when used to describe a substance that binds to a receptor the term agonist refers to a substance that activates the receptor function.
satiety – satisfied in terms of food intake or the state of not being hungry
Questions
1. Sympathetic nervous system discharge
a. elevates blood glucose but reduces blood free fatty acids.
b. elevates blood free fatty acids but reduces blood glucose
c. elevates both free fatty acids and blood glucose
d. reduces both free fatty acids and blood glucose.
2. Beta - receptor stimulation in skeletal muscle results in
a. stimulation of glycogenolysis
b. inhibition of glycogenolysis
c. storage of glycogen
d. none of the above
3. T/F Ephedrine has direct norepinephrine like effects.
4. T/F Chronic administration of aspirin alone has no effect on energy expenditure in experimental animals.
5. The mechanism of action of aspirin, caffeine and ephedrine involves
a. thermogenic actions only
b. anorectic properties only
c. both anorectic and thermogenic properties
d. neither anorectic or thermogenic properties
6. T/F here is strong evidence to suggest that athletes can benefit from supplementation with caffeine, ephedrine and aspirin.
7. T/F Caffeine alone has no effect on metabolic rate.