![]()
RECONSTRUCTION SURGERY
INTRODUCTION
One of the new projects commenced by the Bangkok Biomaterial Center in the last 5 years is the preparation of Human Bone Hydroxyapatite Intra Ocular Orbital Implant for cosmetic anophthalmic correction in Ophthalomology. There are many alternatives to this implant in the surgery and one of them is glass ceramic eye ball. However with artifical implant materials there is always the risk of incompactibiltiy with human tissue i.e rejection by the human body to foriegn material. Also the import cost in Thailand is prohibitive for the common man. This is the place where the Bangkok Biomaterial Center ventures into the research and development of an implant of human origin paid the dividents. Prof. Yongyudh Vajaradul - Chairman of the BBC was of the opinion that if unsterile human bones discarded from various surgeries are treated to high temperatures above 1000 degree celcius, they will be converted to pure hydroxyapatite. Thus with this concept the idea was first carried on at the BBC laboratory on an experimental basis. After satisfying results, these HOA bones were shaped into spheres of different diameters. A preliminary study was conducted on the permeability and susceptibility of the implant to moisture. After getting the desired results, the idea was mooted to a group of expert ophthalmology surgeons in Bangkok, who were very much inclined to give it to clinical trials because references were there that this kind of researches are also being conducted in the US following exactly similar methods. This case is one of the applications of Intra Ocular Implant being prepared by the BBC. However in this case a unique combination was made and it is the first of its kind in the world. The Intra Ocular Implant was wrapped in freeze dried dura mater, sutured and then inserted into the orbital cavity. According to our information till now there is not a singel literature reference in the world about this technique. The concept of using dura mater was the initiation of Prof. Yongyudh Vajaradul, who is of the opinion, that if FD dura mater is utilized in the covering of the implant, then there will be following achieved:
1. Very rare possibility of fibrosis or rejection
2. During the placement of the eye ball surface prosthesis, the intra ocular implant will provide a very stable seating bed.
3. The ends of the dura can be convinently attached to the 6 muscles in the eye which will results in the optimally co-ordinated eye ball movement with respect to the normal eye.
PATIENT DETAILS
Patient Name : Mr. Jigong Moddang
Surgeon Name : Dr. Chalao
Hospital Name : Bangkok Priest hospital
Patient Age : 69 years
Diagnosis : Phthisis bulbi RE / Shallow fornix RE
Date of Surgery : 14/03/2000

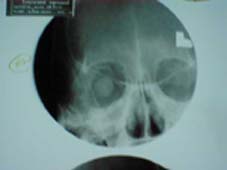
Post operative one week with human hydroxyapatite X-ray post operative one week


Case No. 2 post operative one week. Post operative one week
Case Report: Application of High Temperature Treated Human Bone Hydroxyapatite Intra Orbital Implant Wrapped in Dura mater in Ophthalmology.
Abstract: Intra orbital implants like glass ball has been use for over decades as a cosmetic anophthalmic correction. However one major complications noted with the usage of non-human origin material is infection and non-compatibility of the implant with human body. We at the Bangkok Biomaterial Center (BBC) had developed the high temperature treated human bone hydroxyapatite intra-orbital implant (HHAOI) to be used as a cosmetic correction for anophthalmos. This implant has been in used in Thailand since 1993. We report this case of a 69 years old male Thai patient diagnosed with anophthalmos and shallow fornix in the right eye who was primarily enucleated for several years without any implant. The BBC has supplied the implant along with freeze dried radiation sterilized dura mater. Intra-operatively. The dura mater and HHAOI were soaked in a solution of Gentamycin in Balanced salt solution (BSS). The HHAOI implant was wrapped with the moistened freeze dried dura mater and sutured with 5/0 dexon. The wrapped implant was then pushed into the orbit as deep as possible. Tenon and conjunctiva were then sutured by 5/0 dexon and 6/0 CCG respectively. At a follow-up of 6 months the patient is doing fine with no signs of any complications and custom made ocular prostheses was well fitted. The x-ray of the orbit showed the well centered of the implant but the bone scan showed only mild vascularization of the implant. The prosthesis-motility was not so good because this is the secondary Implantations. The motility may be better after peg coupling along with the prosthesis.
Orbital implants may be divided into three groups: the buried nonintegrated, the buried integrated and the exposed integrated implants.1 The motility of the prosthesis with the buried nonintegrated implants, such as the Mule�s sphere implant, is generally poor. Although Nunery and associates2 recently suggested that suturing rectus muscles to a silicone sphere implant wrapped in autogenous fascia or preserved sclera may enhance the motility. The incidence of extrusion of the exposed integrated implants is unacceptably high. The desire to provide adequate motility as well as to minimize incidence of superficial tissue breakdown and exposure of implants prompted the development of the buried integrated implants. Since their first introduction in the 1940s there have been various designs of buried integrated implants reported. Although the incidence of extrusion was less than that of the exposed integrated implants, the buried integrated implants also had been associated with superficial tissue breakdown and implant exposure, certain implants appeared to be associated with a higher incidence of superficial tissue breakdown or implant exposure than others.3,4 Recently the hydroxyapatite implant has gained much attention. Porous hydroxyapatite was introduced as a buried integrated orbital implant by Perry AC. in 19855, and since its approval by the Food and Drug Administration in August 1989 it has gained increasing popularity.6,7 There have been over 10,000 hydroxyapatite orbital implants placed in patients since May 1985, including eviscerations, enucleations and secondary implants. It is a naturally derived (from marine coral) hydroxyapatite that is very similar in composition to the mineral portion of human bone. It�s micro-architecture is characterized by an interconnected matrix of pores, having an average diameter of 500 ?m. A patented manufacturing process converts the calcium carbonate exoskeleton of the coral to hydroxyapatite (calcium phosphate) via a hydrothermal exchange reaction, while preserving the unique micro-structure of the coral exoskeleton. This porous sphere of calcium phosphate becomes incorporated into the host�s tissue through vascularization.5,8,9 After vascularization of the implant, it may be drilled to provide an attachment for the prosthesis. With drilling and peg placement, hydroxyapatite orbital implants have the advantage of excellent prosthesis motility, considered to be superior to that of other implants; furthermore, they have been associated with very few side effects. The most widely emphasized complication has been implant exposure.10 In Thailand it was first introduced in 1994. It was very success in using this material for the passed five year but with the economic crisis in this part of the world including Thailand push us to look for another substitute that more suitable for our economic status. The objective of this study will be to find the appropriate surgical techniques, as well as to evaluate the advantages and disadvantages of a bone-hydroxyapatite orbital implant and to study the performance of the ocular prosthesis after surgery in Department of Ophthalmology, Priest Hospital, Bangkok10400, Thailand.
Materials and Methods
Bone-hydroxyapatite intra-orbital implantation was performed in a 69 year old male on March 2000 at Priest Hospital, Bangkok, Thailand. He was enucreated for many years, so this is the secondary implantation. �Primary implantation� refers to implant placed at the time of enucleation or evisceration; �Secondary implantation� refers to implant placed sometime after the initial procedure. The implant was hydroxyapatite that was prepared by Bangkok Biomaterial Center. It was made from human bone that treated by high temperature.
Preparation of the implant
The hydroxyapatite ocular implant is nonsterile and must be sterilized by autoclaving in a gravity steam autoclave for 20 minutes at 2500 F (1210 C) or for 10 minutes at 2700 F (1320 C). Alternatively, the implant can be sterilized in a vacuum steam autoclave (pre-vac or hi-vac) for 10 minutes at 2700 F (1320 C). The implant can also be sterilized by ethylene oxide gas sterilization using a gas dwell time of 105 min. at 1300 F (54.40 C) follow by 20 min. of aeration at 1220 F (500 C). It should be soaked in an antibiotic solution, such as gentamycin 80mg in 10 ml. of sterile water for10 min. before being used.
Preparation of dura-mater
In using freeze dried dura-mater, it was well-rehydrated by rinsing with NSS and soaking in an antibiotic solution for 30 minutes before use.
Surgical technique(Secondary orbital implant)
In cases of anophthalmos without orbital implant, the extraocular muscles are difficult to identify and isolate. The pocket inside the orbit is made, the orbit was sized , using a set of sizing spheres , to determine the size of the implant to be used. An implant is of the proper size when it is the largest implant that can be placed deep into the orbit without creating tension on the overlying tissues and while allowing adequate room for an artificial eye of sufficient thickness. The implant may be re-shaped by carving with a scalpel blade. Re-shaping is most easily done when the implant material is wet. Loose particles of hydroxyapatite should be removed from the implant by irrigation prior to implantation. The implant was placed into the orbit by being wrapped in a well-rehydrated dura mater (autogenous or homologous sclera can be used as well). The surface of the hydroxyapatite material is very rough, and a wrapping material facilitates insertion and placement of the implant deep into the orbit. Additionally, a wrapped implant may be more resistant to exposure caused by abrasion from the surface of the implant on the overlying tissues. The 3x5-mm windows were cut in the wrapping material at the site of the attachment of the extra-ocular muscles as well as the posterior aspect to facilitate vascularization of the implant. Then wrapped and windowed homologous hydroxyapatite orbital implant is placed into the orbit as deep as it can.Tenon�s capsule and the conjunctiva were closed in separate layers. In cases of the migrated implants, the existing implant is removed , the pocket is closed layer by layer and a secondary hydroxyapatite implantation is done one to three months later.
Post-operative management
In order to minimize the post-operative hemorrhage and edema, a firm pressure dressing for 7 days. The patient will have severe pain during the first few days of the post-operative period, an analgesic drug combined with a sedative drug should be given beforehand. An antiemetic drug may be necessary in some cases. Antibiotic and anti-edema drugs should be given for one week. About four to six weeks after surgery a temporary prosthesis may be fitted allowing the patient to be un-patched. After three months all the tissues are completely healed. A custom made ocular prosthesis is fabricated. for those who want to enhance motility, a drilling process is prepared after one year. A bone scan is done to confirm vascularization. The patients who had grade 4 of vascularization in the hydroxyapatite orbital implant were selected for drilling of holes for the supporting peg. Drilling the hole in the implant should be done under topical anesthesia combined with retrobulbar anesthesia. Marking the position of hole should be done by using a prosthetic model. The hole is drilled to a depth of at least 13 mm using a cutting bur. A flat head peg was left in the hole for 6 to 8 weeks to allow complete epithelialization of the hole, then the ball-head or ftat-head peg was coupling to the prosthesis.
Result
There were no serious complications from the surgery although there was marked edema caused by intra- orbital hemorrhage which subsided after one week. The swelling subsided within 10 days by using some antibiotic and anti-edema drugs. In follow-up intervals of 6 months there were no extrusion, and no migration of implants. We have seen no unusual orbital inflammatory reaction. We were using 20-mm hydroxyapatite spheres, this left enough room for adequate anterior chamber depth on the prosthesis. The use of an 18-mm sphere may be too small for a normal orbit. There was a marked depression of the superior orbital sulcus. In these cases the prosthesis must be added up to correct the depression. He had been sent for x-ray of the orbit and bone scans after 6 months after operation. The results were shown in fig 1 and 2. The implant was perfectly centered in the orbit. The bone scan showed inadequate vascularization, it was only grade one. The prostheses was fitted 3 months after operation. The motility of the prosthesis was not so good, because this is secondary implantations where extraocular muscles were not identified. The motility may be improved after peg coupling which shouls be done many months from now. The peg coupling was also very good in holding the weight of the prosthesis.
Discussion
While several reports6,7 have documented good success with hydroxyapatite after enucleation . Reporting of experiences with hydroxyapatite for evisceration has been very limited, because of an unfavorable exposure rate of 67% .11 Our experience with evisceration and hydroxyapatite has been more favorable and is the same as Kostick DA, et al12 which reported a rate of exposure of 6%. We have no large exposure except one case that had small erosion of the conjunctiva after 16 months of wearing of the ocular prosthesis and the erosion healed spontaneously.We prefer evisceration with hydroxyapatite over enucleation whenever possible due to better motility. The rate of implant exposure in our series is considerably low. We did not encounter any major complications such as orbital infection, extrusion, or migration of implant and / or sympathetic ophthalmia.
The surgical technique is important in use of hydroxyapatite. The favorable results depend on these major keys. For the proper size of the implant, the bigger the better. The implant can be re-shaped to allow closing wound without tension. The implant should be wrapped securely in the front especially in evisceration. The cornea should be taken out and replaced with scleral patch. The surface of the hydroxyapatie implant is very rough and can be easily exposed if the wound was not closed properly.The confirmative bone scan was done in 11 cases. Four of them had the fourth grade level of vascularization at 9 to 15 months post operatively. The cases with shorter follow-up time had poor vascularization. There were 2 cases at 12 month post-op. whichh had poor vascularization. These cases were over 60 year old and enucleation with homologous scleral wrapped were performed. Other forms of biocompatible implants are being developed, including polyethylene, polytetrafluoroethylene and other forms of porous calcium phosphate implants. Although we presume that these implants would be appropriate, we have no personal experience with them.
Conclusion:
Coralline hydroxyapatite as an ocular implant appears to offer a significant improvement over all previously used materials. The better cosmetic results with fewer potential complications. The long term benefits, as well as the risks remain to be determined. The use of hydroxapatite increases the cost of the surgery along with additional surgical time, confirmative bone scans, secondary drilling procedures and modification of the prosthesis. Nevertheless, the benefits of this material extend beyond its obvious cosmetic value. If long-term studies confirm its lower migration and extrusion rate, and its relative resistance to infection, the medical advantages of hydroxyapatite will make the cost worthwhile.
References:
Gougelmann HP. The evolution of the ocular motility implant. Int Ophthalmol Clin 1970;10:686-711. |
|
Nunery WR, Cepela MA, Heinz GW,et al. Extrusion rate of silicone spherical anophthalmic socket implants. Ophthalmic Plast Reconstr Surg 1993;9:90-5. |
|
Wexler SA, Frueh BR, Musch DC, Pachtman MA. Exposure of tantalum mesh orbital implants. Ophthalmology 1985;92:671-5. |
|
Troutman RC. Symposium: Orbital implants after enucleation. End results of implant surgery. Trans Am Acad Ophthalmol Otolaryngol 1952;56:30-4. |
|
Perry AC. Integrated orbital implants. Adv Ophthalmic Plast Reconstr Surg 1988;8:75-81. |
|
Dutton JJ. Coralline hydroxyapatite as an ocular implant. Ophthalmology 1991;98:370-7. |
|
Shields CL, Shields JA, De Potter P. Hydroxapatite orbital implant after enucleation. Experience with initial 100 consecutive cases. Arch Ophthalmol 1992;110:333-8. |
|
Ferrone PJ, Dutton JJ. Rate of vascularization of coralline hydroxyapatite ocular implants. Ophthalmology 1992;99:376-9. |
|
Shields CL, Shield JA, Eagle RC, De Potter P. Histopathologic evidence of fibrovascular ingrowth four weeks after placement of the hydroxyapatite orbital implant. Am J Ophthalmol 1991;111:363-6. |
|
Nunery WR, Heinz GW, Bonnin JM,et al. Exposure rate of hydroxyapatite spheres in the anophthzalmic socket: histopathologic correlation and comparison with silicone sphere implants. Ophthalmic Plast Reconstr Surg 1993;9:96-104. |
|
Buettner H, Bartley GB. Tissue breakdown and exposure associated with orbital hydroxyapatite implants. Am J Ophthalmol 1992;113:669-73. |
|
Kostick DA, Linberg JV. Evisceration with hydroxyapatite Implant, Surgical Technique and Review of 31 Cases Reports. Ophthalmology 1995;102:1542-9. |