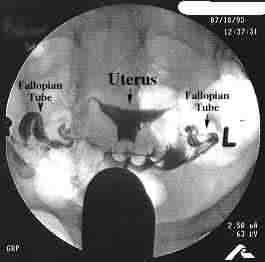
An abnormal HSG may show a problem in the uterine cavity - and this appears as a gap or filling defect.
However, the commonest problems on HSG appear in the tubes. If the tubes are blocked at the cornual end (at the uterotubal
junction), then no dye enters the tubes and they cannot be seen at all. If the block is at the fimbrial end then the tubes
fill up; but the dye does not spill out into the abdominal cavity and the end of the tubes are often swollen up.
Sometimes, like any other medical test, the HSG may provide erroneous results. For example, the cornu of
the uterus may go into spasm, as a result of which the dye may not enter the tubes at all. This may be interpreted as a tubal
block, whereas in reality the tubes are open. Also, if a hydrosalpinx is very thin and if the dye is injected under pressure,
the dye may appear to spill into the abdomen through a tear in the wall of the hydrosalpinx - suggesting tubal patency when
really the tubes are closed.
While the HSG is usually very reliable for determining whether or not the tubes are open, it provides little
information on structures outside the tube which could nevertheless impair tubal function - such as peritubal adhesions. If
the spill is "loculated",(i.e. it collects in small puddles), the presence of adhesions can be suspected, but not confirmed.
An HSG can be painful - and when the dye is injected into the uterine cavity, most women will experience
a considerable amount of pain. You should be prepared for this - and taking a pain-killer prior to the procedure will help
to reduce the pain.
An HSG can be technically difficult for some women (especially if the cervix is too small or too tight)
- and it is better if a gynecologist is present at the time of the HSG to assist the radiologist if needed. Many gynecologists
will do the HSG themselves.
The major risk of an HSG is that of spreading an unrecognized infection from the cervix up into the tubes.
This is uncommon, but in order to reduce the risk, many doctors advise antibiotic coverage during the procedure.
If the HSG shows that the tubes are closed, then it may be advisable to repeat the HSG; and also to do a
laparoscopy to confirm this diagnosis.