4.4
Case Study – Pituitary adenoma
Adenomas
are the commonest primary neoplasms of the pituitary gland.
They are benign and slow growing.
Those smaller than 10mm in diameter are termed microadenomas and
those larger than 10mm are termed macroadenomas.
Approximately 75% of patients with pituitary adenomas will have
symptoms of hormone excess, while the remaining non-functioning tumours,
usually the macroadenomas, present with clinical symptoms related to
tumour mass-effect (e.g. headache, visual field defects, cranial nerve
palsies (Evanson, 2001).
On
high resolution CT scans pituitary adenomas are typically hypodense in
comparison with the normal gland on both contrast-enhanced and unenhanced
images. Similarly, on MRI
80-90% of microadenomas appear as focal hypointense lesions compared with
the normal gland on unenhanced T1-weighted images.
After Gd-DTPA injection the adenoma is seen to enhance less
brightly than the rest of the pituitary gland.
The use of Gd-DTPA increases the sensitivity of MRI in adenoma
detection. Although up to 50%
of microadenomas are hyperintense on T2-weighted images, overall,
T2-weighted sequences are less sensitive than T1-weighted sequences for
the detection of pituitary adenomas.
For this reason they are not used routinely MRI of the pituitary (Evanson,
2001; Rao and Robles, 1999)
Other
evidence of adenoma includes: focal erosion of the sella floor or focal
convexity of the superior surface of the gland. Tilting of the pituitary stalk may also indicate the presence
of an adenoma. Macroadenomas
have similar characteristics to microadenomas and can be reliably and
accurately identified by CT.
Large
solid pituitary macroadenomas appear as masses that are nearly isointense
with the brain in both T1 and T2-weighted images and they enhance
moderately with Gd-DTPA. Cystic,
necrotic and haemorrhagic components within the tumour have intermediate
signal intensity intermediate between that of CSF and that of tumour in
T1-weighted images and have high signal intensity in T2-weighted images. Macroadenomas may grow upwards to compress the optic nerves
and chiasma or may extend downward to the sphenoid sinus, which are best
appreciated on coronal MR images. It
may also encroach on the suprasellar cistern and may displace the optic
chiasm or temporal lobe. It
is important to diagnose cavernous sinus invasion by pituitary adenoma but
unfortunately neither CT nor MRI has proved highly accurate in
preoperative detection. The
identification of tumour lying laterally to the lateral tangent the intra
and supracavernous internal carotid artery on coronal MR images is highly
suggestive of cavernous sinus involvement.
Sagittal MR images are especially useful in demonstrating chiasmal
compression and posterior extension of the tumour (Evanson, 2001; Rao and
Robles, 1999)
Large
pituitary adenomas are prone to develop infarction or haemorrhage owing to
their tenuous blood supply. Pituitary
tumours may also undergo ischemic necrosis if blood supply to tumour is
impaired which may lead to pituitary apoplexy, which can be only
identified at surgery or during MRI (Rao and Robles, 1999)
4.5.1 Patient
This
62-year-old lady presented with the following features:
·
a non-specific headache,
·
decreased visual acuity in both eyes
·
normal pupillary light reaction
·
bitemporal superior quandrantopia (i.e. absence or loss of
one quarter of the visual field)
The
patient had a CT scan immediately performed.
A mass in the sellar region was identified by the radiologist
however, the results were not specific.
The patient was referred for an MRI scan as follows.
Figure
11 Coronal T2-weighted 3mm cut through pituitary
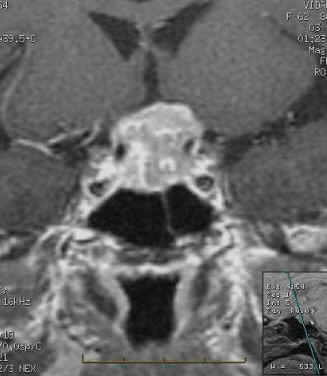
Figure
12 Coronal T1-weighted 3mm cut through pituitary
4.5.2
Materials and methods
The
same materials and methods were used a stated in section 3.5.2
4.5.3
Protocols and pulse sequence parameters
Table
4 Pulse sequences in pituitary MRI
|
Pulse
Sequence |
TR
(ms) |
TE
(ms) |
NEX |
Matrix |
Slice
thickness (mm) |
Slice
spacing (mm) |
FOV |
|
Axial PD FSE (dual echo-1) |
3340 |
28 |
1.00 |
384x256 |
6.0 |
1.0 |
24x18 |
|
Axial
T2 FSE (dual echo-2) |
3340 |
97.8 |
1.00 |
384x256 |
6.0 |
1.00 |
24x18 |
|
Coronal
T1 SE |
440 |
10 |
3.00 |
256x224 |
3.0 |
0.3 |
18x18 |
|
Sagittal
T1 SE |
440 |
10 |
3.00 |
256x224 |
3.0 |
0.3 |
18x18 |
|
Coronal T2
FSE |
3000 |
82.1 |
3.00 |
320x256 |
3.0 |
0.3 |
18x18 |
|
Coronal
T1 SE + Gd-DTPA |
440 |
10 |
3.00 |
256x224 |
3.0 |
0.3 |
18x18 |
|
Sagittal
T1 SE + Gd-DTPA |
440 |
10 |
3.00 |
256x224 |
3.0 |
0.3 |
18x18 |
The
above protocol is similar to the one suggested by Bradley (1999).
In his recommended protocol the axial PD/T2 FSE is not included.
Our center performs this sequence as a general brain check-up for
any pathologies. FSE is used
in this case because it is a fast sequence.
As regards Gd-DTPA administration, the patient was administered a
half dose, as this proved effective in pituitary imaging.
The coronal post-contrast sequence was run first as the contrast
will diffuse from the normally enhancing gland.
3D FSPGRE has been used to image the pituitary, however, magnetic
susceptibility effects from air in the sphenoid sinus often degraded image
quality. Dynamic
studies have been also attempted, as recommended in section 4.4.4.1 with
T1 FSE however; I have seen no particular difference in the resulting
images.
The
protocol utilised by the Massachusetts General Hospital (2002) appears
quite different to our protocol. We
agree in using sagittal and coronal T1-weighted images pre and post
contrast. They also recommend
the use of axial T2 and FLAIR, axial DWI through the whole brain and MRS
if possible. The use of fat
saturation through the sella in the post contrast images sequences is
recommended. As an optional sequence they recommend the use of a T1 axial
through the whole brain.
4.5.4 Results
On
scanning the patient with the above parameters, the radiologist identified
a homogenous contrasting tumour measuring 1.5cm, which is abutting the
optic chiasma. No other focal
lesion was identified. The
tumour is intra-sellar extending to the supra-sellar region.
The tumour is invading the hypothalamus and causing a dilatation in
the left ventricle. The
tumour is encasing the middle cerebral artery.
The tumour probably corresponds to a pituitary macro adenoma.
4.5.5 Evaluation of the examination
The images achieved (figs
11-14) are of good quality. The
patient was co-operative throughout the examination.
The only problem with pituitary examination is scan time due to
number of pulse sequences, contrast usage and moreover, in our center we
use SE which are long sequences.
The macroadenoma enhanced after contrast administration. Nevertheless, areas within the tumour appear less intense than other parts. On discussing this fact with a radiologist, the outcome was that there could be areas of haemorrhage or necrosis within such a large tumour.
Figure
13 Sagittal T1-weighted 3mm section (post gadolinium)
Figure
14 Coronal T1-weighted 3mm section (post gadolinium)